I’m not sure where the last six months went. Well, I do know, but it surprises me that I’ve been less inclined to update here. For the year ahead, I’m setting the intention to keep this journal more current.
So what’s new? Both my Hereditary Cancer Predisposition Panel and Developmental Disorders Panel returned a ‘clean’ status on all counts. My most recent blood draw saw all my markers in the ‘normal’ range for the first time in two years, including iron and ferritin—two important markers for anyone training for longer distance races. These results are enough for my medical geneticist to want to investigate further—my clinical presentation doesn’t match my genetic profile, and that piques the interest of any researcher.
What this all means for my running is mostly good.
I’m not broken …
In parallel to all this investigation under a microscope, I’ve been navigating some more practical issues. In my shoes, it is easy to imagine every twinge or ache is a signal of recurrence. So while I logically knew a podiatrist appointment was likely to reveal a running-related reason for my sore left foot, I found myself tamping down nerves as I sat in the office waiting for my doctor.
In the end, with an X-ray to confirm it, my foot is only a reminder that I’m now 62 and what comes with age and my running habit is osteoarthritis. Sigh. I have a cortisone shot as an option if it becomes more painful, but the conservative approach is clever lacing techniques. That and over-the-counter orthotics are working for the moment.
Hand in hand with sorting out my sore left foot, I developed plantar fasciitis in my right—not a huge surprise if my gait was off from favouring my left. The combination of rest and some trial and error with the above lacing techniques seems to have sorted both issues.
Running on hope
My last blood panel underscored what I’ve been feeling—my counts are finally recovering from active treatment. Since last August, I’ve seen my resting heart rate come down to the high 40s, low 50s, which was my baseline pre-treatment, and I feel less worn out by what is my current hard workout. During the fall racing season, I completed three 5ks, each with progressive improvements in my time and, most importantly, what recovery felt like.
Even better, as I’ve gotten back to better running volume and cross-training in the last month, I’m seeing my body composition shift by gaining muscle and shedding (a little) fat,
(Re)search
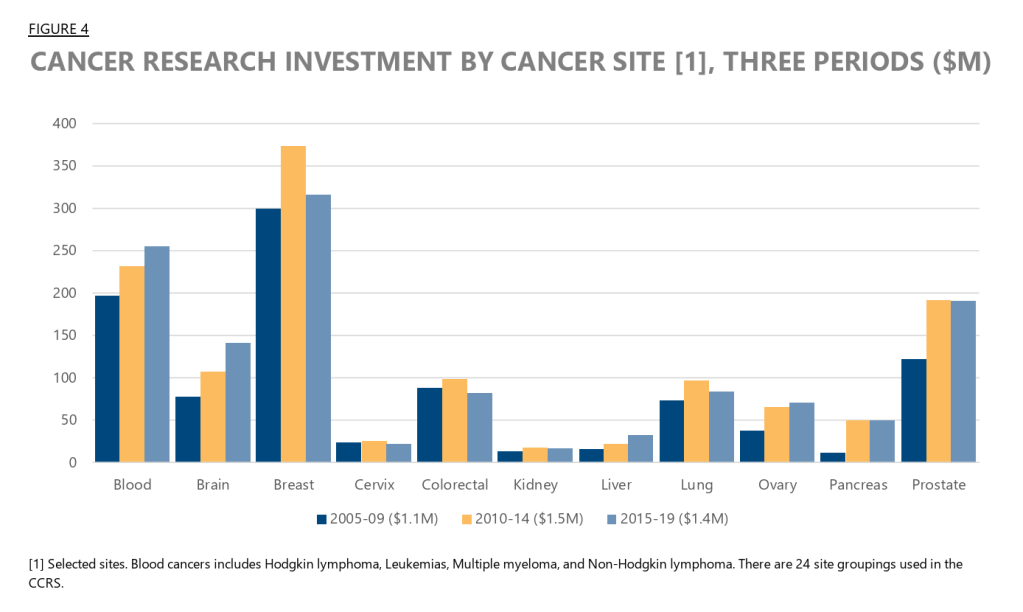
Endometrial cancer is the most common gynecologic cancer diagnosed, and its incidence is rising. Stubbornly, it remains one of the least funded areas of cancer research in Canada. Of the 24 types (sites) tracked by the Canadian Cancer Research Alliance, cancer of the uterus ranks 18/24, and it’s unlikely to register on tables describing where the money goes.
I’m participating in opportunities for cancer survivors to contribute to new research exploring how this disease and its treatment impact quality of life. Lately, that’s meant a lot of Zoom calls.
Making research accessible
When I was diagnosed in November 2023, I quickly discovered that Canada’s clinical trials search engine was ‘under construction’ and redirects pointed to the NIH’s clinicaltrials.gov. With the fragility of healthcare funding in the US under the current administration, it felt like a vulnerable resource.
Recently, cancertrialscanada.ca launched. It is the only ‘national, bilingual, patient-centric website dedicated to cancer clinical trials.’ I had the opportunity to provide feedback on the site before its official launch. A collaboration between the Canadian Cancer Society (CCS) and the Quebec–Clinical Research Organization in Cancer (Q-CROC), the site’s patient-centric approach is a step towards making dense medical research documentation accessible to those who use the content most frequently.
Where does exercise fit?
The Cancer Rehabilitation Team at the University of Alberta conducts research on the intersection of exercise and cancer survivorship. Dr. Shirin Shallwani is a post-doctoral fellow, physiotherapist, and lymphedema therapist exploring physical activity and rehabilitation strategies.
Dr. Shallwani’s study, Rehabilitation and Exercise for Advanced Cancer Health (REACH), focuses on adults living in Canada with advanced or metastatic cancer, and whether current rehabilitation and exercise services meet our needs. My contribution included completing an online survey and group discussions.
What I like about Dr. Shallwani’s work is that it looks at gaps from a patient perspective. I’m especially interested in whether she is looking at patients and survivors seeking guidance beyond the baseline of 150 minutes of exercise/week to mitigate the risk of recurrence.
And what about medications and impact on quality of life?
Canada’s Drug Agency (CDA) provides government expert, independent advice on drug, health technology, and health system decisions. They make recommendations on whether drugs should be covered by Canada’s public health insurance.
This cycle, they are deliberating public coverage of Avastin (bevacizumab), a drug sometimes used to treat advanced endometrial cancer like mine. As part of their work, they invite patients to share their story — what it’s like to navigate treatment options, the impact of limited access, and what matters most to patients with this diagnosis.
When you’re a patient, understanding the side effects, especially rare ones, is crucial in making informed treatment decisions. For Avastin, one of those is osteonecrosis, or dying bone, usually in the jaw. It’s an unpleasant experience that a member of my support group discovered when she had to deal with an unrelated dental problem.
Sharing my story with the CDA is one more way to advocate for patients’ perspectives on managing this disease.
A new training plan
Between all these Zoom calls, I’ve started a new training plan for a spring 10k. A year ago, I imagined I’d be running longer distances by now, and that my world with a year of remission behind me would be similar to what it was before I was diagnosed. I’m learning that ‘going back’ isn’t a useful framing, so this training block is about measuring progress from where I am vs where I used to be. It’s not always an easy mind shift. I’m encouraged that my legs seem to be responding more quickly. When I compare year-over-year training data, my ‘easy run’ these days is a harder workout than last year’s, so I’ve moved the needle on my base, and a 10k in late April, early May, feels attainable again.
Tracking progress, or not
Side-by-side with a training schedule is my new surveillance schedule. Slowly, I’m wrapping my brain around the reality that while my appointments with my radiation oncologist and gynecologic oncologist get further apart with time, I’ve added a whole new set of appointments that will continue in perpetuity. Here’s the surveillance protocol:
- Breast: 2x annually, alternating mammogram with breast MRI
- Thyroid: annual ultrasound and biopsy as required
- Kidney: annual or biannual ultrasound if my regular CT scan for cancer surveillance is discontinued
- Colon: every 5 years from baseline; more frequent if polyps are found
- Skin: Annual exam at the oncogenodermatoses clinic
So this is what ‘normal’ looks like in my immediate future. For now, it’s almost above 0°C and sunny on a Valentine’s Saturday afternoon, so I’m headed outside for a short run. ❤️

Leave a comment