I really wanted to be boring for a while. But oh well.
A few weeks ago, while waiting on pathology, I was musing about my colonoscopy results being ‘the other cancer shoe.’ Well, shoes do come in pairs, so I shouldn’t have been surprised when my doctor confirmed my colon lesion was malignant. To be precise: “Invasive poorly differentiated colorectal adenocarcinoma, BRAF Positive, dMMR, MSI-high.”
Two primaries. One body. Zero chill from my cells, apparently.
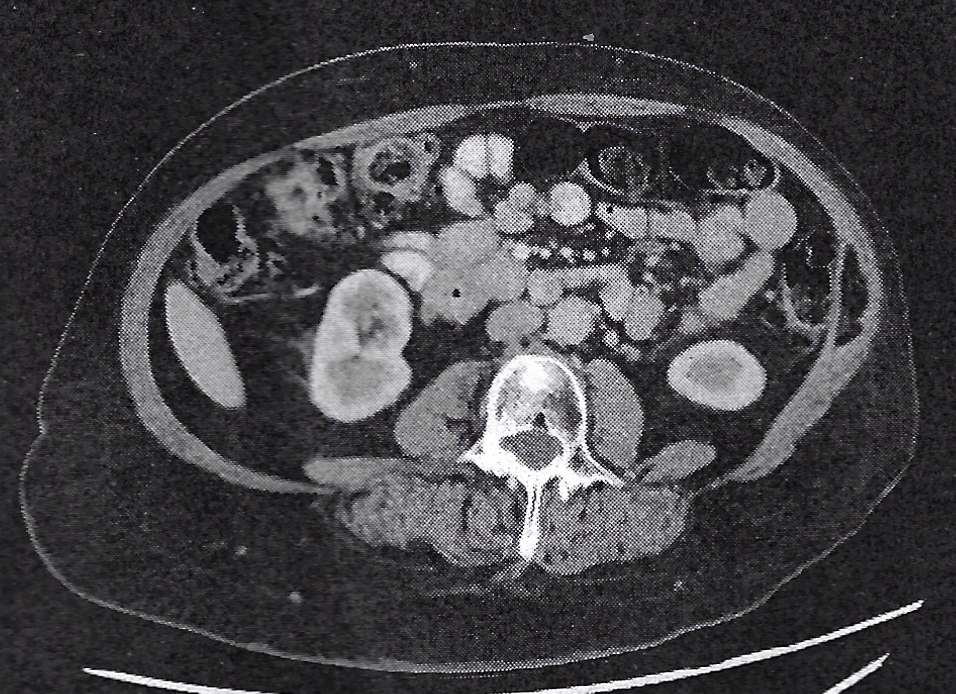
I can tell you now that hearing your second cancer diagnosis is nowhere near as terrifying as the first. I’m not making light of it, but ‘I know how this goes, I’ve done this before,’ did run through my head as a first reaction. It helped that my surgeon was excited: while it is an aggressive tumor profile, it is exceptionally responsive to immunotherapy, and were it not for my Cowden-like diagnosis, with a complete response to treatment, there would be an argument to forego surgery. Add to that, my CT made it clear this wasn’t metastasis from my endometrial cancer, and I consciously exhaled.
As I write this, I’m sitting in the waiting room waiting for a follow-up meeting with my surgeon. This, after seeing my gynecologic oncologist last Friday, and my medical oncologist on Monday. Phew, and it’s only Wednesday.
I’ll be starting immunotherapy in a few weeks, followed by a hemicolectomy—the removal of the right side of my colon. Life is an adventure.
Running is medicine
In parallel to running this gauntlet of appointments, I’ve been on a deep dive learning about my tumor, the biomarkers affecting its behaviour, the immunotherapy I’ll undergo, and the surgery that will follow. And interested to know how that will all intersect with my running habit. After all, it’s not so long ago that my bloodwork finally inched into normal (at least for me) territory, and I started dreaming about races longer than 5k.
My new treatment path and the physical legacy of my endometrial cancer treatment made me concerned. Despite celebrating a normal blood panel in September, my lymphocytes have been persistently on the lower end, and my last blood draw in February reported an elevated fasting glucose. It could have been an outlier, but it also could be a signal of late effects from my chemo. I really didn’t want complications that could constrain the preferred treatment for this new diagnosis.
What I’ve learned along the way is that my running habit has been doing some heavy lifting that is medicinal, as well as being an anchor to my approach to self-care. It turns out that exercise, and running in particular, mobilises your lymphocytes and, by extension, increases the efficacy of your immune system, even when your levels may be below standard. So while my levels have been ‘off’ in the 18 months post-treatment, my running has been doing the work of making them more effective than what might first appear.
Now, I really should strength train
Since January, I’ve been focused on rebuilding muscle mass — fine-tuning my diet and vowing to add regular strength training to my routine. True confession time, the food side has shown results, but my approach to anything other than time on feet and basebuilding could best be described as haphazard.
My two cycles of immunotherapy aren’t likely to be affected by that, but how I navigate a second major abdominal surgery and the recovery will definitely draw on my physical fitness, especially the state of my abdominal wall. Things as simple as getting out of bed are far easier when your lateral abs have some muscle memory.
The good news is that thanks to my running habit, my resting heart rate is in the mid-50s, and my average respiration falls in the 10-12 breaths/minute range. That gives me good cardiac and pulmonary reserves, which align more closely with someone at least a decade younger than I am.

Cue the robots
The topic for today’s meeting is surgery planning. I’m lucky that my clinic is within a leading hospital, and my surgeon pioneered the robotic colorectomy program here. Moreover, she leads the prehab program as well. That means that while she’s said for her it’s a matter of scheduling whether my surgery is laparoscopic or robotic, she welcomes my preferences on the topic.
For me, it’s not just that a robotic procedure has a shorter recovery window; it’s also that it means less disruption to my abdominal wall. A hemicolectomy is a more complex procedure than my hysterectomy and BSO. The ascending colon is in close proximity to major vasculature that requires care and attention. It will follow six weeks (2 cycles) of immunotherapy, which adds complexity to a surgical field already constrained by my prior radiation. And the anastomosis (reconnection of the parts of my bowel after they remove the section where the tumor made its home) carries risk. A robotic approach not only allows my surgeon more dexterity and precision, but it also means it will all happen intracorporally (inside the body) versus having a 7 cm incision to pull the parts of my bowel outside my body and sew them back together.
Toeing the line one more time
I’ve had to let go of my dreams of a spring and fall race season—again. Next weekend, I’ll run the Beneva 8k Spring Runoff virtually as my first and last race before this new treatment cycle. Instead of being a test of my fitness for longer races in the fall, it will serve as a baseline to gauge how well I navigate and recover from treatment.
Running and recovery
As with my previous surgery, the recommended window to return to running is 6+ weeks, or, in running terms, ‘one week more.’ I’ll likely feel like I’m ready to run before my body has fully caught up with my brain, so the adage to ‘add one more week’ once my brain says ‘go’ is good advice. It’s not that different from any distance race: don’t go out too hard—advice I’ve never been particularly good at following.
Now it’s just a matter of getting dates firmed up for when treatment starts. And a lot of ab work to make sure my core is ready for what’s to come.

Leave a comment