I’m one week post-surgery, officially POD8, and sitting in the sun on a Saturday afternoon. I was discharged from the hospital on Wednesday and, if I’m being honest, this recovery has been something of a roller coaster. You never know until you’ve been through the treatment how your body will absorb the trauma, and mine has some strong opinions, it turns out.
The body keeps score
That intro sounds a little melodramatic for what has, in the bigger picture, been a straightforward recovery so far. But my frame of reference for surgery is my 2024 hysterectomy, when I wasn’t even admitted and slept in my own bed that night. This time, I’m two years older, with six rounds of CarboTaxol and twenty-five EBRT treatments under my belt (literally). All relevant details about how my body is responding this time around.
My surgery was first on the schedule, and I was in PACU by mid-day. I was in my room and eating dinner—shepherd’s pie (yes, really)—by the end of the day. My surgeon told me everything went well and that she’d see me on Monday. I sent a few emails and texts to let everyone know I was OK, then drifted off, attached to an IV for fluids.


What happened next is that I woke up around 3:30 a.m., clammy and in pain. Pressing the call button didn’t summon the night nurse (plug for better staffing levels all around), and it was 5:30, and time for new vitals, before I got some relief. Vitals showed I was running a low-grade fever, and my CRP—C-reactive protein—had spiked to 324. Individually, neither is concerning; together, they may be an early sign of a complication or infection. My hope of an early discharge vanished because blood cultures to rule out infection take 48 hours to mature. Ah, well, it was the weekend at least.
In the end, the fever and the spike were nothing more than a natural way to manage the physical trauma of surgery. I do think my body’s response was also a sense memory from chemo and radiation, dialling its reaction up to 11 based on previous interventions. It may also have been compounded by my lower WBC going into surgery. With fewer white blood cells, my body marshaled a higher signal to ensure my immune system was as efficient as possible.
As quickly as my CRP and temperature climbed, though, they retreated from that peak almost as fast. The next day, I was still a little warm, but my numbers were trending in the right direction. By Wednesday, with cultures clear and CRP falling steadily, I was discharged. Home, favorite chair, Tylenol, and some sun.
The weird stuff nobody mentions
One of my post-op surprises has been subcutaneous emphysema. Unlike the usual gas under your diaphragm, this is when air leaks under the skin, mostly across your neck and chest. It’s harmless and temporary, but it’s like having a thin layer of bubble wrap across the area, and “harmless” isn’t the first word that comes to mind when you can make the same popping sounds by running your hand over your chest. Bodies are weird.
Training a new gut
The bigger adjustment—the one I’m still in the middle of—is bowel changes. I went into this surgery well-informed. I asked questions. I read. I understood, intellectually, that removing my ascending colon would change how my gut processes food, water, and electrolytes. But understanding it and living it are two very different things.
The unpredictability is more extreme than I expected. I’m learning what I can eat, when, and what the consequences might be on any given day. It’s not linear. Some days are fine, and some days are definitely an experiment. The best analogy I have is that it’s like training your gut for a race—you’re building a relationship with a system that has its own ideas about timing and tolerance, and you have to adjust as you go. Oddly, my favorite chews are useful here to make sure I’ve got carbs and electrolytes onboard.
This is also where I think there’s a real gap in how we prepare active patients for surgery like this. The clinical information I received was solid on the basics—what to expect in the hospital, how to manage pain, and when to call. But nobody talked to me about what bowel unpredictability means, not for my day-to-day, and definitely not for returning to running.
It’s not the fitness side—I know how to rebuild mileage. It’s the logistics side. When you’re planning a run, you need to trust your body on a pretty fundamental level, and right now that trust is something I’m rebuilding from scratch. It’s the kind of conversation that athletic patients shouldn’t have to figure out on their own. It definitely shouldn’t come as a surprise. One resource I’ve found, once I got home, is produced in Australia. It’s candid and practical, and has been the best read for what was happening in the first week I’ve been home. Armed with practical information, it’s easier to be an active participant in your own recovery, instead of just a passenger in the process.
Building a dashboard
It turns out my Garmin has been a truly useful tool as I navigate this week. I’ve been watching my HRV, stress levels, and Body Battery the way I’d watch them during a training block—except this time, I’m not training. I’m mostly draped over my favorite comfy chair. And the data still shows how much work my body has been doing beneath the surface: elevated stress, suppressed HRV, Body Battery draining even when I haven’t moved. Healing is a metabolic load in itself, and my watch confirms it in real time. Gradually, I’m starting to see some light—the blue bars—that show I’m moving from the acute post-surgery phase to a longer-term recovery window.
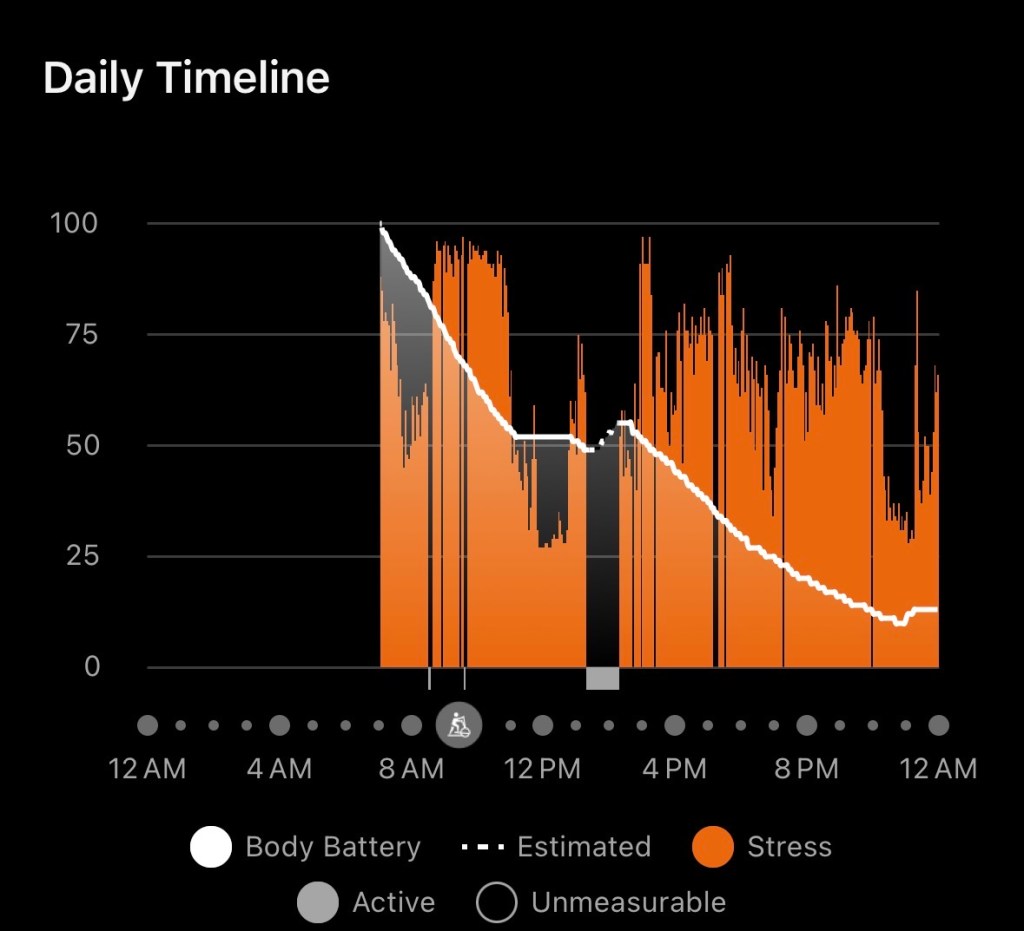
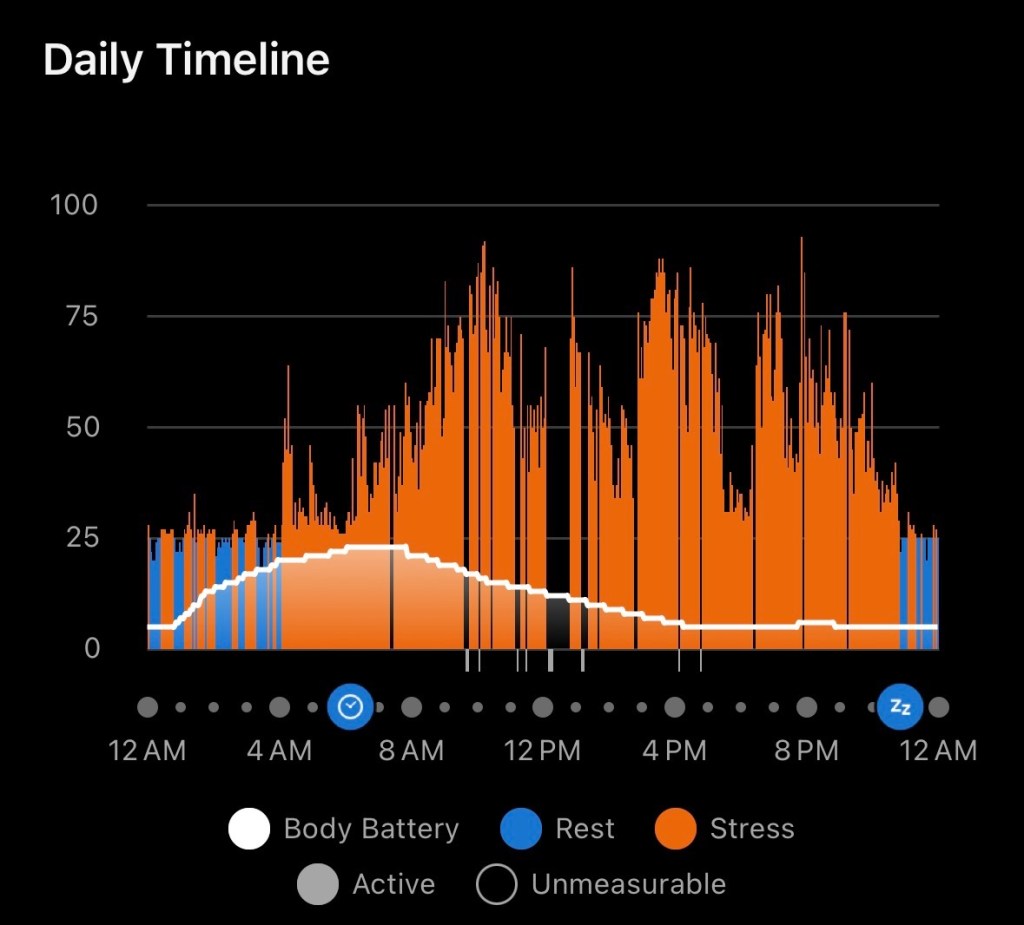
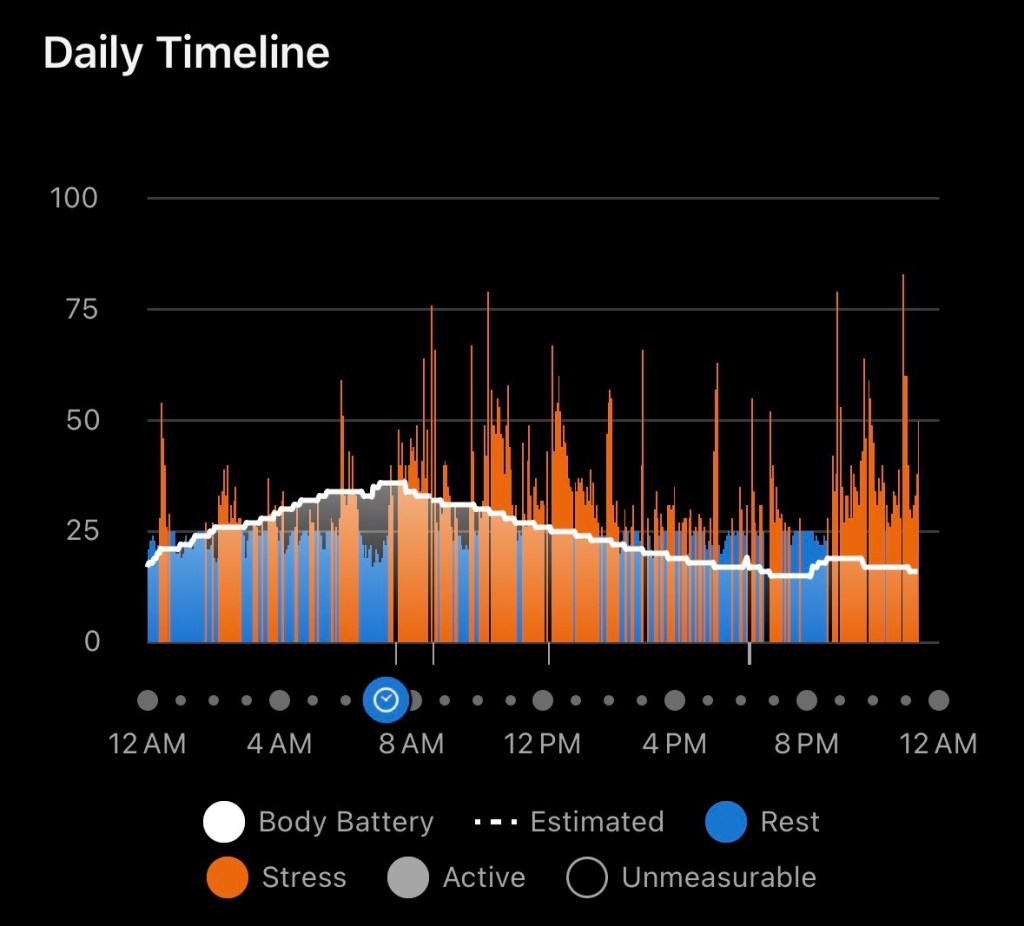
My Garmin tells the story of my body finding equilibrium.
It’s also a good check on my instincts. I’m someone who wants to do more, sooner. My Garmin is a quiet, objective reminder that my body is already doing plenty—it hasn’t yet cracked 50 as a peak, even after a decent night’s sleep, so I’m biding my time before I test my boundaries.
The body does keep score. Turns out, so does my watch.

Leave a comment